Beyond Mandatory Autonomy: Truth Without Abandonment
Honesty and hope aren’t opposing forces. They are a matched set: hope for the best and prepare for the worst—paired with an explicit promise of nonabandonment.


Prognostic Awareness and Hope
Many of us tiptoe around prognosis like it's nitroglycerin: don't jostle it or the whole room blows. The result is familiar—vague timelines, hedged language, and a lot of "let's see how you do." We tell ourselves this is kindness. It is not. It is abdication. It leaves patients unprepared, families guessing, and clinicians complicit in a silence that serves no one except the person who doesn't want to have the conversation.
And that person, more often than we'd like to admit, is us.
Here's the data we don't talk about enough: physicians are accurate in survival predictions only about 20% of the time, with a systematic bias toward overestimation—by a factor of 3 to 5. The longer you know the patient, the worse your accuracy gets. The closer the relationship, the more optimistic the estimate. Your bond with the person in front of you is actively distorting your clinical judgment, and we have known this for over two decades.
That would be concerning enough on its own. But the downstream consequences are where it gets truly dangerous.
The Architecture of Avoidance
Prognostic avoidance isn't a communication failure. It's a system. It has structural supports, cultural reinforcements, and an ethical alibi.
The training gap. A national survey found that while 90% of physicians believed they should avoid giving specific prognostic information, 57% felt inadequately trained in prognostication itself. Read those numbers together: the vast majority of doctors think vagueness is the right approach, and more than half acknowledge they don't actually know how to do the thing they're being vague about. We have built a professional culture where not knowing how to prognosticate and not wanting to prognosticate reinforce each other in a closed loop.
The autonomy alibi. This is where it connects to the argument we've been building across this series. Autonomy doctrine—the version I called "mandatory autonomy" in Part 1—gives clinicians a ready-made justification for silence. "I don't want to take away their hope." "They didn't ask." "I'm respecting their wishes." But autonomy without information is a fiction. You cannot exercise self-determination about a future you don't know is coming. Withholding prognosis in the name of autonomy is like handing someone a ballot with the candidates' names blacked out and calling it democracy.
The collusion. Jane Weeks and colleagues published a study in the New England Journal of Medicine in 2012 that should have changed practice overnight. Among patients with metastatic lung or colorectal cancer—cancers for which chemotherapy is not curative—69% and 81% respectively did not understand that their treatment was not going to cure them. That's bad. Here's what's worse: patients who rated their physician's communication as excellent were more likely to hold inaccurate beliefs about cure. The better they felt about the conversation, the less they understood the truth.
An ethnographic study cited in the same paper identified the mechanism: "collusion" between patient and physician, where both parties quickly transition from discussing prognosis to discussing treatment, refocusing attention and generating false optimism. Treatment becomes the instrument of prognostic misunderstanding. We don't tell them the truth; we tell them the plan. And both parties feel better about it—right up until the plan stops working and there's no time left to do the things that actually mattered.
The incentive structure. No one gets an RVU for telling the truth. There is no billing code for "sat with a family for forty-five minutes and said the hard thing clearly." The system rewards procedures, interventions, and throughput. It does not reward presence, directness, or the conversation that changes everything. Sixty percent of medical oncologists prefer not to discuss code status, advance directives, or hospice until there are no more treatments to offer. Half of all patients with lung cancer reach two months before death without anyone mentioning hospice. These are not communication failures by individual clinicians. This is a system designed to avoid the conversation until avoidance is no longer physically possible.
The emotional cost to clinicians. Nearly 60% of physicians report that making survival estimates is "difficult" and "stressful." This is real, and it deserves acknowledgment rather than dismissal. Prognostic conversations are emotionally expensive. They require sitting in uncertainty, tolerating distress—the patient's and your own—and accepting that the relationship might feel different afterward. The system offers no structural support for that cost. No protected time. No debriefing. No acknowledgment that this is among the hardest clinical work we do. So clinicians absorb it individually, and individually they cope—often by avoiding.
What the Evidence Actually Says
Here is where the mythology collapses.
The belief that prognostic honesty destroys hope is not supported by evidence. The Coping with Cancer study found that patients who had end-of-life discussions experienced no higher rates of depression or worry, had lower rates of ventilation and resuscitation, and entered hospice earlier. More aggressive care near death was associated with higher rates of major depressive disorder in bereaved caregivers.
Among hemodialysis patients, receiving prognostic information was associated with empowerment and hope—not the destruction of it. When discussions didn't happen, patients' fears for the worst actually threatened hope more than honest conversation did. Ninety-three percent of surrogate decision-makers for mechanically ventilated patients considered avoidance of prognostic discussion an unacceptable way to maintain hope.
Read that again. The people we're supposedly protecting by staying silent are telling us that the silence itself is the harm.
It's possible—and I think likely—that hope derives not from what we tell people, but from the relationship in which we tell it. When you sit with someone, look them in the eye, share a difficult truth, and then promise to stay, hope isn't destroyed. It's redirected. It shifts from "maybe this treatment will cure me" to "my doctor will not abandon me." The second kind of hope is sturdier, more useful, and more honest. And it is our job to build it.
The Frame That Works
Honesty and hope aren't opposing forces. They are a matched set: hope for the best and prepare for the worst—paired with an explicit promise of nonabandonment. When we anchor prognostic conversations in nonabandonment—your ongoing, explicit commitment to stay—we reduce the harm of hard news. That obligation is not optional; it's core medical ethics.
The practical target: accurate + tolerable. Pair clear information with structures that help people absorb and use it.
Steal from the best
I'm not asking you to reinvent the wheel. The tools exist. They're evidence-informed and they work. The problem has never been the tools; it's been the will to use them.
Ask–Tell–Ask. Ask what they understand and how much they want. Tell the minimum necessary in plain language. Ask for teach-back. Simple, scalable, and it works. "What's your understanding of where things are?" … "Here's the headline." … "If you were telling your sister what we discussed, what would you say?"
Hope/Worry. Pair hope with your clinical worry and give a range—time, function, or uncertainty. This protects hope while enabling preparation, and people prefer it. "We like to hope for the best and plan for the worst." "I hope this buys you months; I worry it may be weeks."
Ask permission. Patients and families rarely feel a sense of agency. Informed consent is laden with power dynamics and rarely performed with authentic curiosity. Use it sparingly, and asking for permission can be a powerful focusing tool. "After hearing what you're hoping for, may I share with you my thoughts." (Kyle tip: say it and shut up for a moment.)
Nonabandonment. "Our team is here with you. We will keep adjusting as things change." This is the sentence that holds the rest together. Without it, honesty is just bad news. With it, honesty becomes a scaffold.
Use hope typology to tailor your language
Patients "do" hope differently. The following typology is a clinical tool, not a pathology. It helps you match how you talk to what they need.
Technical Hope.
Signal: "What are the odds? What's the best-case worst-case?"
What to do: Offer ranges with best/typical/worst, plus your recommendation. Patients prefer wider ranges paired with "hope/prepare."
Phrase: "Given what we're seeing, I'm hoping for months, and I worry it could be shorter. Here's what I recommend so your care matches what matters to you..."
Spiritual Hope.
Signal: Beliefs, meaning, or faith language anchors their coping.
What to do: Ask what gives strength; invite chaplain or faith leader if desired; avoid debating beliefs. Reach for your Serious Illness Conversation Guide.
Phrase: "What gives you strength as you think about the future? Would it help to bring that person or community into our planning?"
Minimalist Hope.
Signal: Prefers the fewest details needed to plan next steps.
What to do: Use Ask–Tell–Ask to calibrate information load; name your commitment; keep updates brief and regular.
Phrase: "Would it be okay if I give you the headline and then we decide what to do next together?"
Pragmatic Hope.
Signal: Focus on control, logistics, and preparation.
What to do: Pair "hope for best/prepare for worst," give concrete next actions. End your sentences in periods, not question marks.
Phrase: "I'm hoping you keep having good mornings. I'm worried stairs will get tougher. Let's order the equipment now so you're ready."
Under all of this, Janoušková's Hope Theory reminds us that hope blends "agency" (will) and "pathways" (ways). Your job is to support both—even when the pathways narrow. Especially then.
Where I Might Be Wrong
- Cultural variation is real and I've underweighted it here. Preferences for prognostic disclosure vary across cultures. Korean American and Mexican American patients, for example, have been shown to be less likely than African American or European American patients to believe a terminal prognosis should be shared directly. Asking "how much do you want to know?" is a guardrail, not a loophole—but the way we ask, who's in the room, and whether a professional interpreter is present all shape the answer. I'm writing from my corner of the globe and in a English-language, autonomy-heavy clinical frame. That frame is not universal and this piece doesn't fully account for the patients it doesn't fit.
- The evidence base is disproportionately cancer-focused. Most of what we know about prognostic accuracy and prognostic communication comes from oncology populations. Heart failure, COPD, dementia, and neurological disease carry vastly different trajectories, different uncertainties, and different cultural expectations. The tools I'm recommending here are transferable in principle, but the evidence supporting them is narrower than the clinical reality where you'll use them.
- Structural change requires more than individual clinician behavior. I've framed much of this piece around what you can do tomorrow. But the incentive structures, training gaps, and time pressures I named in the "Architecture of Avoidance" won't change because individual clinicians get better at one conversation. Systems redesign—protected time, billing reform, mandatory prognostic training, debriefing infrastructure—is where the durable fix lives.
- "Middle knowledge" is not denial. Patients oscillate between awareness and retreat, often within the same conversation. That oscillation is adaptive, not pathological. If I've made this sound too linear—assess understanding, deliver truth, move forward—the real clinical experience is messier, more iterative, and requires more patience than any framework captures.
The Harder Thing Is the Better Thing
Say the quiet part clearly. Pair it with hope that's real. Make a promise you keep.
Prognostic awareness is not a hammer; it's a hand on the rail so people can walk the stairs. When we offer ranges instead of riddles, name our worry without stealing hope, and say out loud that we won't leave, we stop performing care and start practicing it. We trade euphemism for dignity. We give people time to do the things that still matter.
So this is the ask: stop tiptoeing. Use the few sentences that change the room. Ask what they understand. Tell the headline. Name your hope and your worry. Give the best-typical-worst. Recommend the next right step. Promise to stay—and then show back up.
The "how" is below. Read it. Steal from it. Teach it.

Back to Our Playbook
1) Map values + hope style
Ask verbatim: “What matters most if time is short?” Document exact words. Then tag the dominant hope approach: Technical (more treatment), Spiritual (meaning/faith), Minimalist (comfort, less intervention), Pragmatic (time at home, function). Early, structured goals‑of‑care conversations improve alignment, family outcomes, and reduce non‑beneficial care near death.
2) Set the Kon dial
Offer a stance choice: recommendation vs equal partnership vs non‑dissent for non‑beneficial options. Say it out loud: “Some people want my recommendation; others want to decide together.” Make explicit that any recommendation reflects the patient’s values, not yours.
3) Build awareness iteratively
Use Ask‑Tell‑Ask: assess understanding → share tailored info → check back. Pair Hope/Worry/Wonder: “I wish for more time; I worry CPR won’t help you leave the hospital; I wonder if we can focus on comfort and home.” Document current prognostic awareness and expect “middle knowledge” (oscillation between hope and realism).
4) Check bias/power
Name mistrust, language needs, and your positional power. Invite correction: “If I miss or misinterpret something, please stop me.” SDM struggles in the hospital include uncertainty, time pressure, fear of losing control; surface them so you can manage them.
5) Pivot when flooded
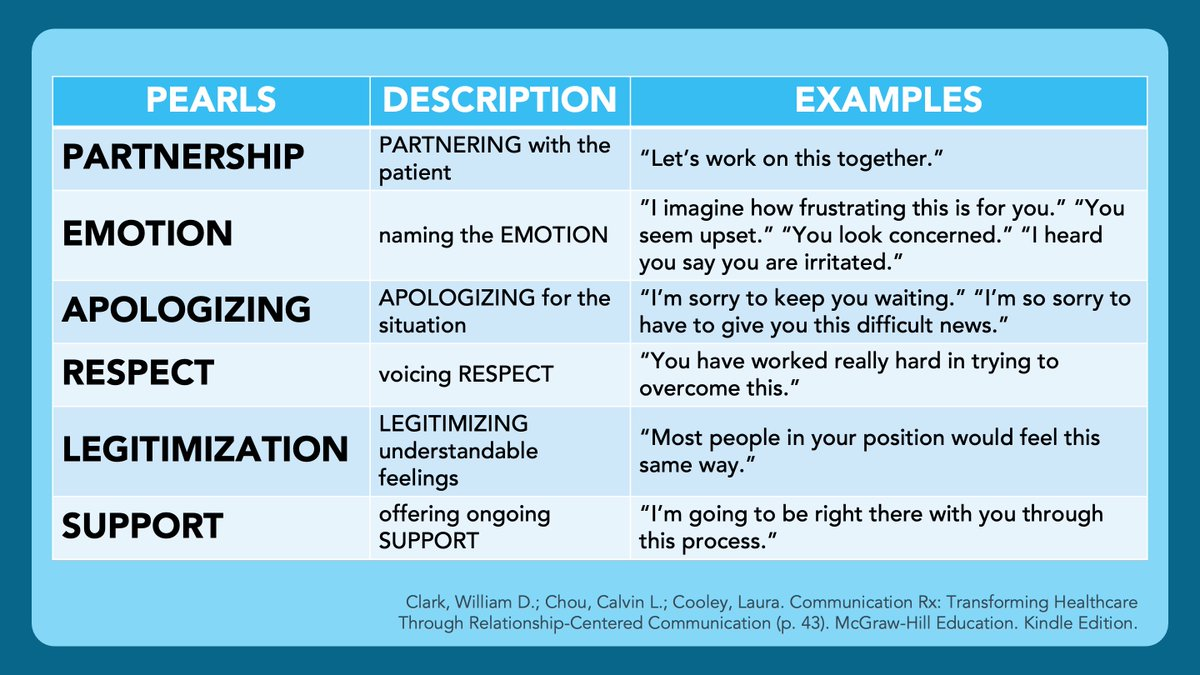
If open‑ended questions backfire, switch to structured clarity: short declaratives, explicit compassion, and focused options only. Use PEARLS skills (never NURSE, that acronym is terrible) alongside Ask‑Tell‑Ask to regulate emotional bandwidth.
6) Highlight the best choice (the maternalistic move)
When trust is strong, values are known, and the patient wants guidance, present a package deal aligned with goals with an off‑ramp to dissent: “Given what matters to you, my recommendation is no CPR, comfort‑focused care, and discharge home with hospice. If that feels wrong, say so and we’ll adjust.”
This is recommendation inside SDM, not coercion.
7) Use informed non‑dissent for non‑beneficial CPR
Elicit values → explain why CPR won’t achieve those ends → state a caring assessment → invite disagreement. Trials are testing this approach among older, seriously ill adults, and ethical analyses support its use. Local law/policy varies; know your institution’s stance.
8) Align orders with goals
Stop offering interventions that cannot reach the patient’s stated ends. Replace checkbox code talks with values‑anchored care plans.
I am a palliative care physician, educator, and professional strategery expert. Known for turning rounds into rants and rants into teaching points. Rounds & Rants represents my views — not those of any institution or professional membership organization where I hold a role. I don't write on their behalf and they don't vet what I publish.



