Teams, Not Saviors: Protecting Each Other from Compassion’s Edge States
Every team thinks they’re compassionate. Fewer can name the cliffs embedded in compassion—and fewer still can stop one another from going over the edge in the middle of a messy consult.


Medical education has an empathy problem. Not too little of it. Too much of the wrong kind, taught without the scaffolding that makes it safe.
You know the video. The animated bear climbs into the fox's dark hole and says "I know what it's like down here, and you're not alone." It's Brené Brown's RSA short on empathy, it's been viewed hundreds of millions of times, and it is shown in medical schools, nursing programs, chaplaincy training, and palliative care fellowships with the frequency and reverence of a liturgical text.
I'm here to tell you it's not quite right (yikes, that is intimidating to write).
Brown gets the sympathy-empathy distinction right. But her framework stops at the edge of the cliff. Empathy—unregulated resonance with another person's suffering—is not the destination. It's the on-ramp. And if you teach people to merge onto that highway without also teaching them to steer, brake, and pull over, you are training them for a wreck.
Joan Halifax has a better map. Where Brown draws a binary (sympathy bad, empathy good), Halifax draws a continuum with a cliff in the middle:
Sympathy = "I feel for you...from here. That must be hard...over there."
Empathy = "I feel with you; your suffering resonates in me."
Compassion = "I'm with you and I am not you; I let your suffering flow through me, keep my footing, and take the next helpful step."
That middle term—empathy without the "and not you"—is where clinicians get hurt. Teaching medical students to be empathic (mad scientist voice: align those mirror neurons, children, what could go wrong!?) without also teaching them how to discern self from other, regulate their internal state, and choose something prosocial to do with those feelings is a recipe for empathic distress. In my opinion, it is a dangerous path that too many medical educators lead students down without a return ticket.
The formula is straightforward: Attention + affect regulation + prosocial intention → wise action.
Skip a step, and you get overwhelm, withdrawal, or coercive interventions dressed up as caring. We've all seen it. Some of us have been it.
Halifax's Corrective
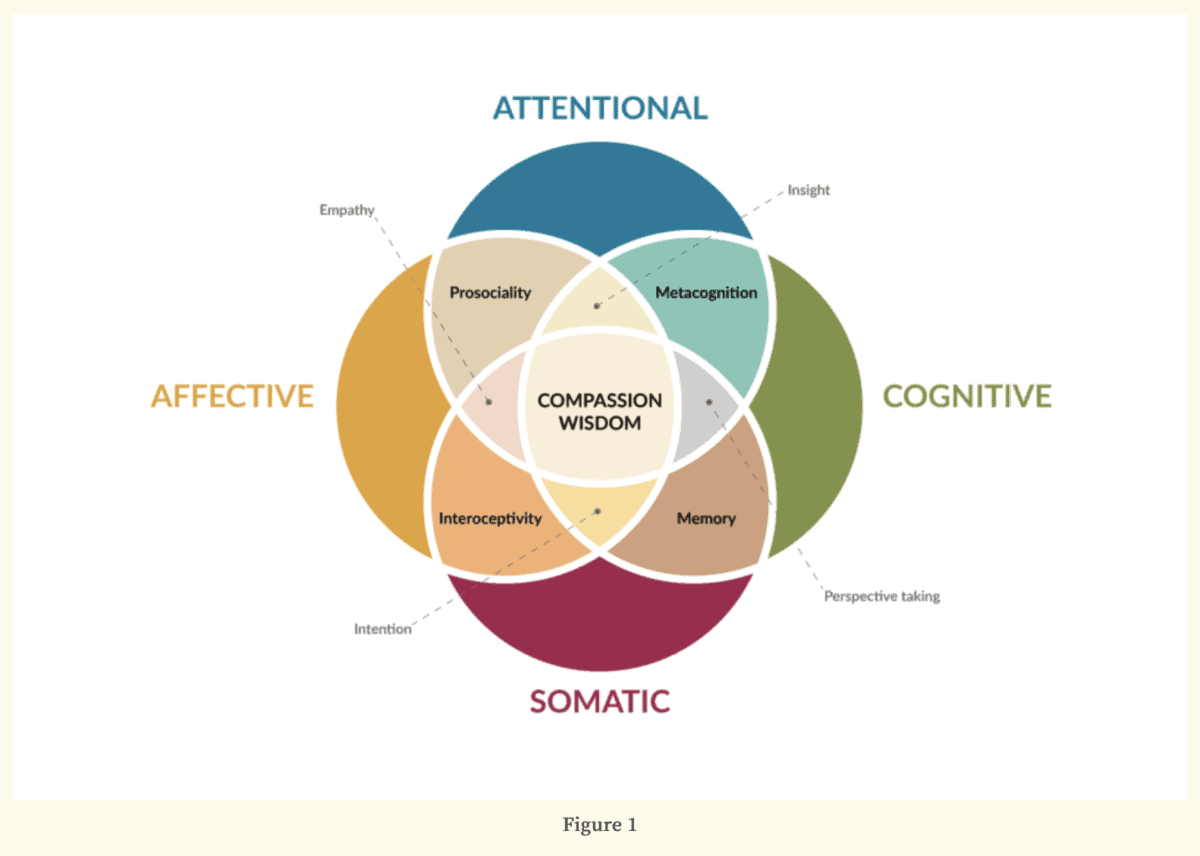
Halifax spent her time as a Distinguished Visiting Scholar at the Library of Congress building what she calls a heuristic model of enactive compassion and then refined it over the coming years. The key insight: compassion is not a feeling you summon. It is a process you enact—attention, affect, intention, insight, and embodiment working together in real time. Each element is trainable. None of them is empathy alone.
She also names five capacities that enable this process—and, critically, each capacity's shadow when it tips over:
- Altruism ⇄ pathological altruism. Service becomes rescuing, saviorism, or self-sacrifice that harms the patient, the team, or you.
- Empathy ⇄ empathic distress. Resonance floods, numbs, or drives you to control the family to stop your own discomfort.
- Integrity ⇄ moral distress/injury. You can't do what you believe is right; cynicism and outrage take the wheel.
- Respect ⇄ disrespect/objectification. Paternalism masquerading as efficiency; "we know best" replaces eliciting values.
- Engagement ⇄ overwork/burnout. Endless to-do lists, eroded efficacy, collapse.
I'm old now, apparently, so I like to say things like "I prefer it the way it was." And that's true here, where I find myself more compelled by Halifax's earlier, provocative language around Wounded Healers and the Shadow States of Caregiving in Being with Dying: The Hero, The Martyr, The Parent, The Expert, The Priest. Those names land in a clinical team's gut faster than a taxonomy does. And each one carries its own antidote: share the responsibility, build resilience, cede control, face uncomfortable feelings, practice not-knowing.
Let's move on to where this stops being theory and starts being Tuesday afternoon.
Code Status as a Mirror
Is this just because I find any chance I can to bring up Nathan Gray's code status cartoons? Maybe! Deal with it!
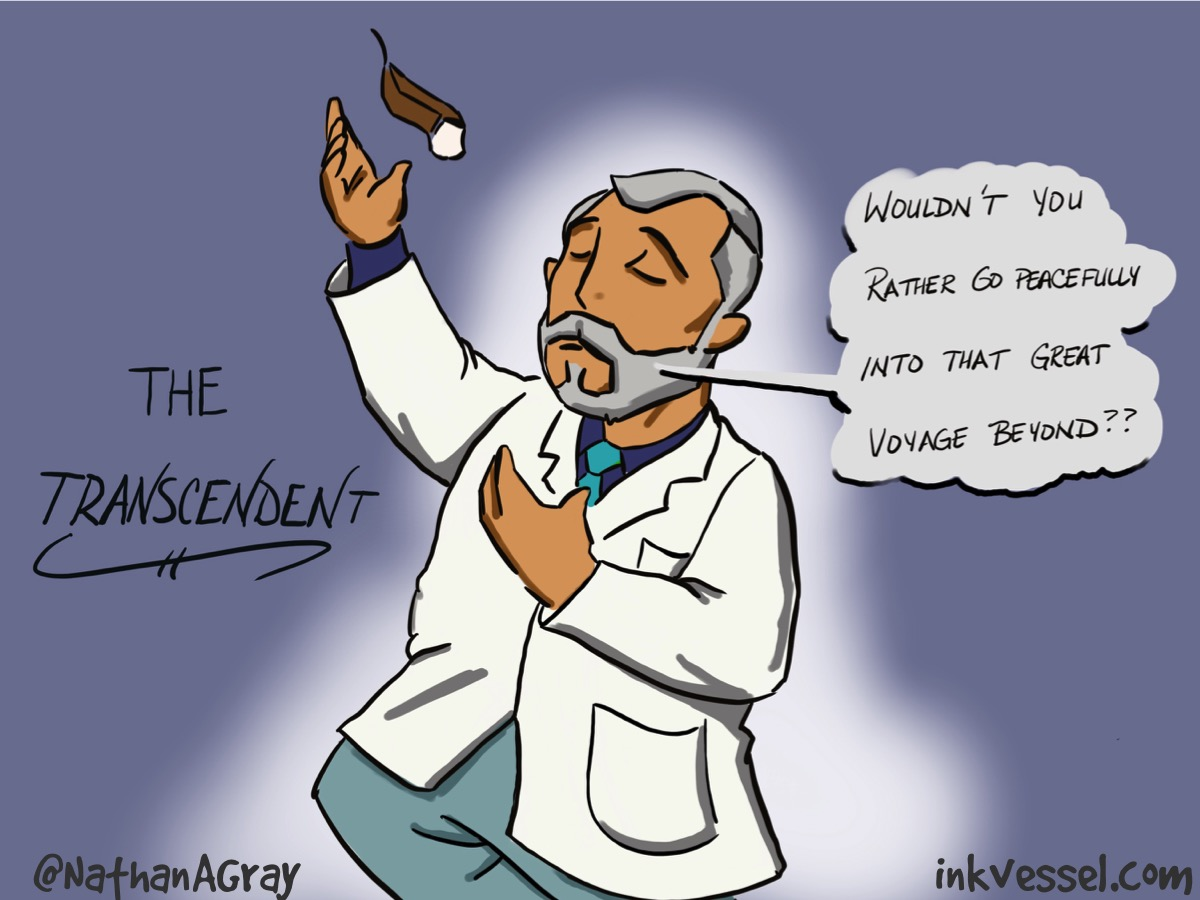
Nathan names common approaches to code-status conversations—"The Menu," "The Transcendent," "The Horrors," "The Numbers," "The All-or-None"—and offers a pragmatic "3 C's" mnemonic (Context, Concerns, Code). Most people read his work as communication coaching. I want you to read it as edge-state diagnostics. Because every anti-pattern Nathan drew is a compassion shadow in disguise.
"The Menu"—dumping options, abdicating guidance—signals disrespect (treating people as decision-machines rather than meaning-makers) and overwork (clinician bandwidth so taxed that scaffolding meaning gets skipped entirely). When we offer the menu, we're not being neutral. We're being absent.
"The Transcendent"—projecting metaphysics onto the patient—slips into disrespect by presuming beliefs and can reflect pathological altruism: imposing what we think will "help" as a way to ease our distress, not theirs. In San Diego Hospice lingo, this is "advocacy before inquiry." It feels like compassion. It's the opposite, it's manipulation.
"The Horrors"—scare tactics about CPR, graphic descriptions of rib-cracking and intubation—is classic empathic distress masquerading as patient education. The clinician is flooded with their own fear and discomfort, and passive-aggressively attempts to move the patient where they want them to be. This is not informed consent. It's emotional contagion pointed at the most vulnerable person in the room.
"The Numbers"—statistical barrage about survival rates and outcomes—can reflect moral distress avoidance. The data is a bunker. All those numbers and big words function like a nice, weighted MedEd blanket I can cozy up under as a physician—warm, familiar, and utterly disconnected from the human sitting across from me who is trying to figure out what their life means.
"The All-or-None"—binary framing, "everything or nothing"—erodes respect and integrity simultaneously. It implies that choosing comfort means choosing abandonment. It is neither honest nor patient-centered, and it persists because it's fast, it's simple, and it relieves the clinician of the harder work of navigating uncertainty with someone.
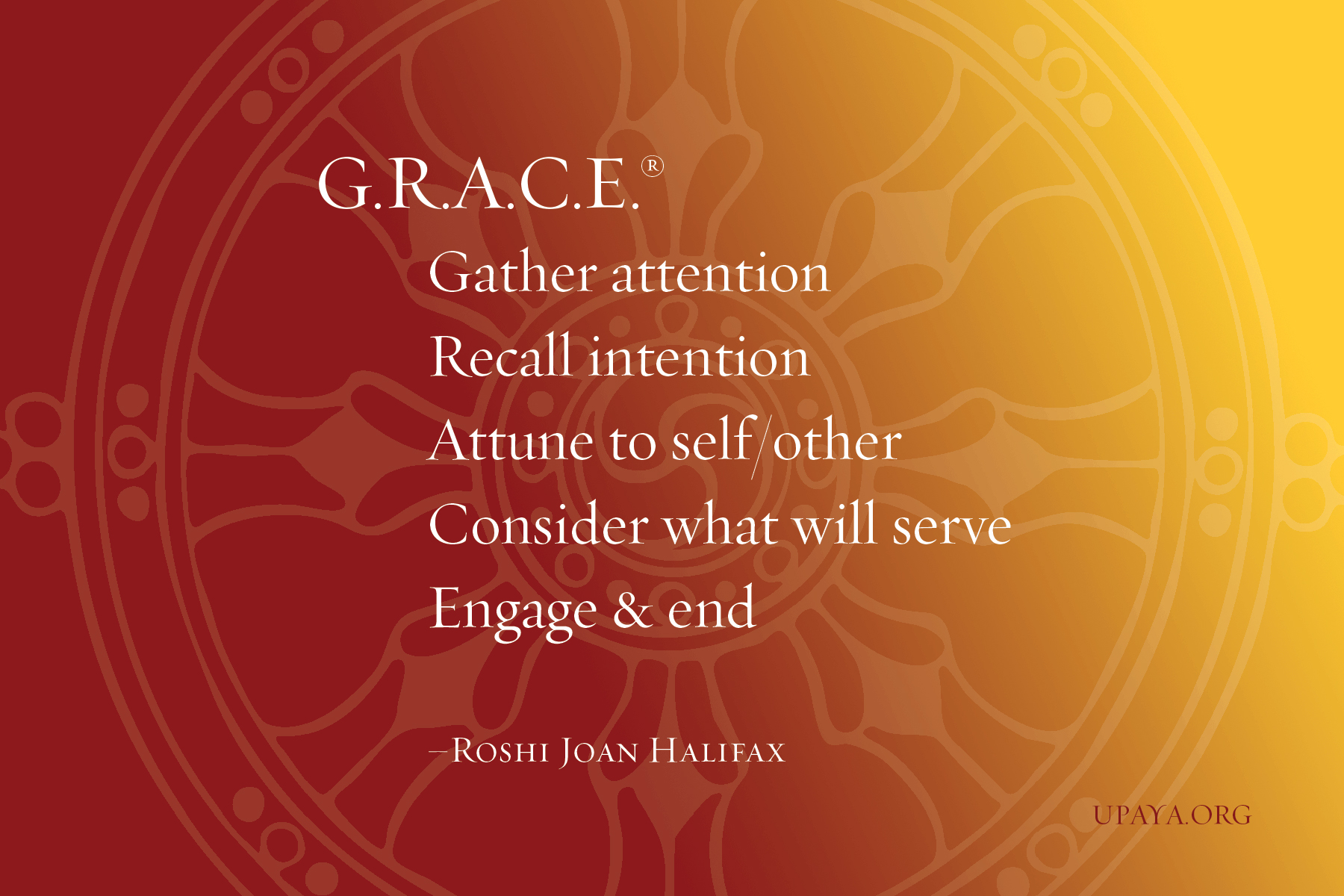
Nathan's 3 C's are an applied antidote to these shadows. Start with Context (the Gather and Recall of G.R.A.C.E.), name Concerns (Attune and Consider), then discuss Code (Ethically engage)—all while regulating your own empathic load.
The point is not that code status conversations are uniquely shadowed. The point is that they're diagnostic. If you can learn to see which edge state is driving a bad code conversation, you can learn to see it everywhere: in the family meeting that went sideways, in the team member who can't let go, in the charting that documents tasks but erases values. The framework doesn't change the content of your work. It changes what you notice about how you're doing it.
What the Shadows Look Like Outside the Code Conversation
Once you have the lexicon, you start seeing edge states in the fabric of daily practice. Here's what to watch for on your team—including in yourself.
Pathological altruism sounds like "my patient" and "my family." It looks like declining offers to co-lead, taking on extra visits "because they need me," scope creep disguised as kindness. The antidote is naming shared leadership for the problem at hand: who leads this—PharmD, SW, Chaplain, Physician? Set a boundary and a handoff in the room. Articulate the next smallest helpful action, then stop.
Empathic distress sounds like rapid speech and "we need to decide now" when there's no clinical trigger for urgency. It looks like menu-dumping, post-encounter numbness, crankiness that seems out of proportion. The antidote—and I recognize this is cheeky, but I mean it and I live it—is a really good personal therapist. The micro-level intervention is a 60-second G.R.A.C.E. pause before the next question: Gather attention, Recall intention, Attune to self/other, Consider what will serve, Ethically engage. Seriously, take this training. It is excellent. And consider making G.R.A.C.E. your team's "safety pause"—a 60-second pre-brief before difficult encounters and a 60-second debrief after. Pair teammates as "GRACE buddies" authorized to call the pause when anyone is sliding.
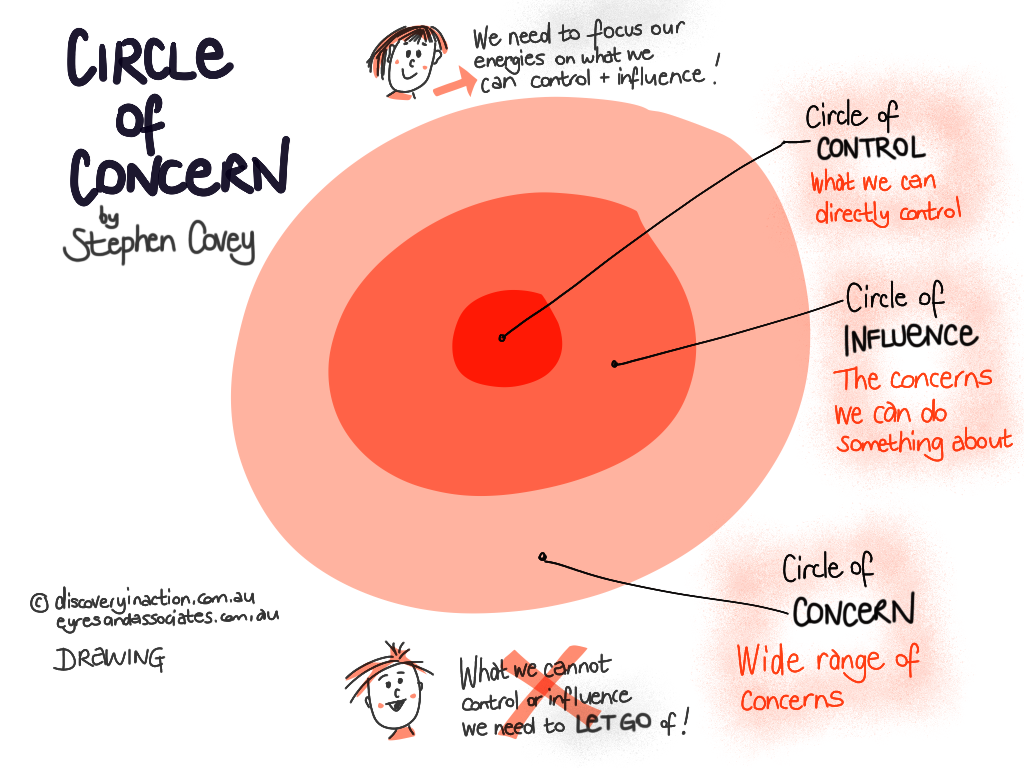
Moral distress sounds like "what's the point?" It looks like avoidance of the primary team, sarcasm that has stopped being funny, charting that lists tasks but avoids values. The antidote is naming the conflict—values vs. system—and giving language to the circles of concern. (The most important Venn Diagram in the whole world.)
Disrespect sounds like fewer questions and more declaratives. It looks like translating goals into clinician language rather than eliciting them in the patient's own words. The antidote: lead with values first. Elicit meaning before proposals. Mirror the patient's words verbatim; only then translate to clinical options.
Burnout sounds like "I'll just do it myself." It looks like skipped breaks, calendar double-books, a mounting pile of small oversights. The antidote is structural, not motivational: daily five-minute load-rebalancing huddles, automatic buddy assignments for complex tasks, one protected no-meeting hour per discipline.
None of these are character failures. All of them are predictable consequences of training people to resonate without teaching them or giving them tools and time to regulate.
Physician Perspective (Without Re-centering Physicians)
I've written about the physician's counter-cultural role on specialist palliative care teams. What the edge-state framework adds is a sharper picture of the physician's specific shadows.
Physicians are trained to be The Expert. We're rewarded for it. And The Expert shadow—retreating into the neocortex, hiding behind data and big words, repackaging SW or chaplain insights as "medical" to maintain control—is our most comfortable failure mode. It's also Brené's Armored Leader in action (see, I still love your work, Brené!). We need to come down out of the neocortex and face uncomfortable feelings. That is the work.
What physicians owe the team: translate risk and trade-offs for other physicians while amplifying discipline expertise—don't repurpose someone else's insight to show off. Model disciplined uncertainty—Halifax calls this the practice of not-knowing—so the team can be honest without paralysis, then still act. I happen to be fond of the term "strong objectivity." Whatever you call it, we can be sure that certainty belongs (almost?) nowhere in the practice of palliative care. Intervene decisively on real physician problems (refractory symptoms, safety, high-risk pharmacology), then step back and protect team learning.
The Point
Go back to where we started. The problem is not that clinicians lack compassion. The problem is that we've spent two decades teaching people to feel with their patients without teaching them to stay upright while doing it. The result is predictable: empathic distress disguised as dedication, moral injury disguised as resilience, pathological altruism disguised as going above and beyond. We reward the crash and call it caring.
Halifax's framework is the corrective. Compassion is not a feeling you perform. It is a process you enact—attention, affect, intention, insight, embodiment—in real time, with a team that shares the language and has permission to intervene when someone is sliding.
That's what high-functioning specialist palliative care looks like on Tuesday at 4:15 p.m., when the current consult is wild and the chats won't stop. It's not more heroes. It's not more empathy workshops with animated bears. It's teams that know the terrain, name the shadows, and keep each other from the cliff.
Compassion is not fragile. It's precise. And it's ours to practice.
I am a palliative care physician, educator, and professional strategery expert. Known for turning rounds into rants and rants into teaching points. Rounds & Rants represents my views — not those of any institution or professional membership organization where I hold a role. I don't write on their behalf and they don't vet what I publish.



