You Will Not Be the Person Who Filled Out That Form
What if the reason ACP underdelivers isn't that we do too little of it, but that we've misunderstood what it's for? The answer lives in an unlikely place for a clinical field: behavioral economics.


CMS recently proposed a quality measure that would tie reimbursement to whether patients have documented advance care planning conversations. The measure—MUC2025-020—would apply to hospitals, home health agencies, skilled nursing facilities, and ambulatory surgery centers, and fold into MIPS. The framing is familiar: $200 billion a year spent on care patients say they wouldn't want. Only 36% of American adults have documented their end-of-life wishes. Everyone nods. Everyone agrees this is a problem worth solving.
They're right that it's a problem. We have to shape the approach to make it meaningful. If the outcome is making advance care planning a quality checkbox doesn't just fail to solve the underlying problem—it generates a new one. When you incentivize documentation over dialogue, you get documentation. Not understanding. Not preparation. Not better decisions in the moment they matter most. You get a field in an EHR and a billing code and a false sense that something meaningful has occurred.
What if the reason ACP underdelivers isn't that we do too little of it, but that we've misunderstood what it's for? The answer lives in an unlikely place for a clinical field: behavioral economics. And it turns out that the way humans actually make decisions under uncertainty isn't just relevant to ACP—it's devastating to the entire checkbox paradigm.
The Checkbox and the Conversation
To be clear, the instinct behind MUC2025-020 is sound. Too many patients receive unwanted care at the end of life (which, of course, is only truly clear retrospectively). Too few have had any conversation about what matters to them when they're seriously ill. Systematizing that conversation isn't a bad impulse. The problem is what gets systematized.
The measure could be as simple as requiring tracking whether ACP documentation exists in the electronic health record. Koda Health's Chief Medical Officer, Desh Mohan, told Hospice News that the documentation requirements "have not been fully defined or shared" and warned that "check box approaches often are not effective." He's right. But the concern goes deeper than implementation details.
The article's dominant framing is cost savings. A venture capital investor in Koda Health and former CMS chief technology officer, framed the opportunity as "a no-brainer" for saving money across the board in health care. ACP-as-cost-reduction is ACP with the patient extracted from the center. Yes, aligning care with preferences often reduces spending. But the moment you build a quality measure around cost avoidance rather than decisional quality, you've built the wrong thing. You've incentivized the documentation of preferences, not the preparation of human beings to navigate uncertainty.
And uncertainty, it turns out, is the entire game.
The Debate You Probably Know About
Before we go further, some context. In 2021, Sean Morrison, Diane Meier, and Robert Arnold published a viewpoint in JAMA titled "What's Wrong With Advance Care Planning?" Their argument was blunt: three decades of research and $300 million in funding have produced weak, low-quality evidence that ACP achieves its core objective of goal-concordant care. Morrison compared the field's continued investment to his family's efforts to fix a fundamentally flawed Ford Pinto. Stop pouring money into a broken model, he argued. Redirect resources toward symptom management, care models, and systems that actually deliver.
Rebecca Sudore, Susan Hickman, and Anne Walling responded that Morrison was attacking a version of ACP that the field has already moved past. The evolution from document completion to iterative, communication-based preparation for in-the-moment decision-making is real, evidence-based, and ongoing. Dismissing all of ACP because early studies of advance directives showed little impact is like dismissing all of oncology because early chemotherapy regimens were brutal.
Both sides had a point. Morrison was right that the dominant version of ACP—the one CMS is now proposing to incentivize—doesn't reliably produce goal-concordant care. Sudore was right that a more sophisticated conception of ACP, one focused on preparing patients and surrogates rather than pre-specifying treatment preferences, shows genuine promise. The CMS measure, as currently described, appears to be incentivizing the version Morrison correctly identified as broken while ignoring the version Sudore has spent two decades building.
I want to push this further than either of them did, by asking why the checkbox version fails. Not "the evidence is mixed." Not "implementation varies." Why, structurally, is asking healthy people to document future treatment preferences a fundamentally flawed approach to medical decision-making? The answer is prospect theory.
How Humans Actually Make Decisions
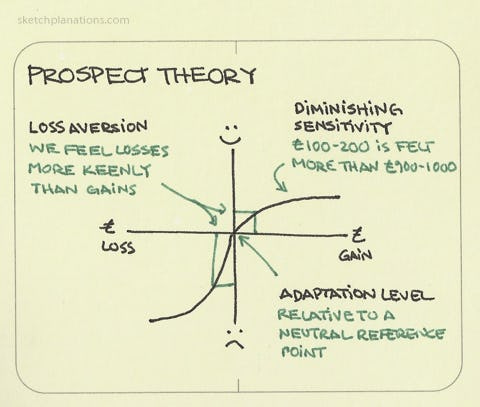
Daniel Kahneman and Amos Tversky developed prospect theory in 1979 to describe how people make decisions under conditions of uncertainty. It has been one of the most consequential contributions to behavioral science in the last half-century. It has reshaped economics, public policy, and marketing. It has barely touched palliative care.
A 2014 JAMA Viewpoint by Verma, Razak, and Detsky distilled prospect theory into a three-step heuristic for physicians. First: people simplify choices by focusing on key differences between options and ignoring similarities—the isolation effect. A patient weighing chemotherapy will fixate on survival length, quality of life, and side effects, while disregarding things like the need for palliative care or advance directives, which will matter regardless of what they choose. Second: people select a reference point from which to frame their decision. In medicine, this might be their current health, a memory of past health, or an expectation of future health. Third: people estimate the overall value of their options based on how pleasurable or painful an outcome is expected to be and the probability of its occurrence.
Every step of this heuristic presents a problem for checkbox ACP.
Consider the reference point. Verma and colleagues describe an elderly man with advanced non-small cell lung cancer deciding whether to pursue non-curative chemotherapy. The internist's reference point is the patient's current poor health—she sees potential gain from baseline and prefers the certainty of 8.5 months without chemo's side effects. The oncologist and family use a different reference point—the chance to survive 15 months—and see the decision as a potential loss from that possibility. They're willing to accept the risks of chemotherapy to avoid losing that chance.
Same data. Same patient. Radically different decisions depending on where you stand when you look at them. (And humans HATE to make themselves responsible for choosing a loss.)
Now consider what checkbox ACP asks people to do: select treatment preferences without a clinical reference point at all. A healthy 65-year-old completing an advance directive at their annual physical is making a decision about a hypothetical future from a reference point that has almost nothing to do with the reference point they'll occupy when the decision actually matters. They're not simplifying a real choice; they're imagining one. They're not framing a decision from their current illness experience; they're projecting from wellness into a state they have never inhabited.
A Harrington and Kerr study in Health Communication (2017) makes this more specific. They replicated and extended the original Tversky and Kahneman disease-outbreak experiment to test whether consequence severity—the variable that health communication researchers had been treating as the driver of risk-based decisions—actually mattered. It didn't. Across two experiments with 1,300 participants, what drove decision-making wasn't how severe the consequence was but how certain the outcome was. Participants preferred certainty when outcomes were framed as gains regardless of whether the disease was deadly or easily curable, and showed no clear preferences at all when outcomes were framed as losses.
This matters for ACP because most advance directive questions are framed around severity: "If you had a terminal illness…" "If you could not recognize your loved ones…" "If you were in a persistent vegetative state…" Prospect theory and its empirical descendants suggest that severity is the wrong variable. What will actually drive decision-making in the moment is the uncertainty of the clinical situation—the probability that an intervention will produce a meaningful outcome—and the reference point the patient occupies when the decision is being made. Neither of these can be known in advance. Both are invisible to a checkbox.
Why "Do Everything" Isn't a Preference
There's a finding in the Harrington and Kerr data that deserves more attention than it gets. In Kahneman and Tversky's original experiment, prospect theory predicts that people will be risk-seeking when outcomes are framed as losses: faced with certain loss, they'll gamble on the uncertain option. That's the classic result. But Harrington and Kerr didn't find that. In their loss-framed conditions—both deadly and easily curable scenarios, across both experiments—participants showed no clear preference at all. Not risk-seeking. Not risk-averse. Decisional stasis.
This is clinically devastating. Serious illness is almost always a loss frame. Once you're sick, every option is defined relative to what you've already lost or stand to lose further. And Kahneman and Tversky's original work tells us that losses loom roughly twice as large as equivalent gains in subjective experience. The pain of losing something you have is psychologically more powerful than the pleasure of gaining something you don't. Apply this to the bedside: choosing to forgo life-extending treatment is an active decision to accept a certain loss. Continuing disease-directed treatment—even when the probability of benefit is vanishingly small—requires no active decision at all. It is the default. It is the status quo. It is what happens when you do nothing.
The psychological weight of these two positions is not symmetrical, and this is where the omission bias compounds loss aversion. People judge harmful actions as morally worse than equally harmful inactions, even when the outcomes are identical. A surrogate who consents to withdrawal of life-sustaining treatment is making an active choice that results in death. A surrogate who says nothing—or who says "do everything"—is allowing the medical system to continue on its default course. The first feels like causing a death. The second feels like letting nature and medicine take their course. The moral and psychological burden of those two positions is radically different, even when the clinical outcome is the same or worse for the patient.
This is why "do everything" is not, in most cases, a considered preference. It is what happens when loss aversion and omission bias converge on a surrogate who has not been prepared for the decision they're being asked to make. It is the predictable result of a system that treats the continuation of aggressive treatment as the passive default and the acceptance of death as an active, morally loaded choice. And it is precisely what happens when the only ACP a family has is a checkbox in an EHR that says "conversation documented" without any evidence that the surrogate was prepared to bear the psychological weight of deciding under conditions of loss.
Morrison raised the alarm about this during COVID, when advance directives specifying "no CPR, no mechanical ventilation" were being implemented in emergency rooms for older adults with a virus that turned out to be survivable for some of them. The documents were followed. The conversations were not had. That is the checkbox working exactly as designed—and producing exactly the wrong result. A prepared surrogate with decisional leeway would have asked the right question: "Is this the situation my father was imagining when he filled out that form?" A form in an EHR cannot ask that question. A human being, who has been prepared for in-the-moment decision-making, can.
The Default That Shapes the "Choice"
It gets worse. Halpern, Loewenstein, Volpp, and colleagues demonstrated in a 2013 Health Affairs study that default options in advance directives directly influence what patients choose. They randomly assigned 132 seriously ill patients to complete one of three advance directive forms: one pre-checked toward comfort-oriented care, one pre-checked toward life-extending care, and one standard form with nothing checked. Seventy-seven percent of patients in the comfort-oriented default group retained that choice. Among those defaulted to life-extending care, only 43% switched to comfort. The standard form landed in between.
The implication is uncomfortable: patients may not hold deep-seated, stable preferences about end-of-life care at all. What they "prefer" is, in part, an artifact of how the form is designed. The architecture of the document is doing decisional work that we're attributing to the patient. (Here I'm looking hard at you, SNF admissions teams who have pre-filled full code POLST forms as part of your admit paperwork!)
When CMS proposes a quality measure based on whether ACP documentation exists, they are measuring the presence of a form. That form has defaults—explicit or implicit, in its structure, its language, its ordering of options. Those defaults shape the "preferences" that get documented. And then we call those preferences the patient's autonomous wishes and build a system to honor them. This is a house built on sand, and making it a quality measure pours concrete on top.
The Ship of Theseus Problem
The ancient Greeks posed a thought experiment: if you replace every plank of a ship one at a time, is the resulting vessel still the same ship? The standard version is about identity and material continuity. The version I care about is clinical.

Serious illness replaces planks. The body you had before the diagnosis is not the body you have six months into treatment. The independence you assumed was permanent turns out to be contingent. The relationships that once operated on certain terms renegotiate themselves around new realities—adaptation, dependency, caregiving, anticipatory grief; lost & found & new & deeper friendships. The person who filled out that advance directive in the waiting room of their primary care physician's office is not the same person lying in the ICU years later. Humans' collective superpower is adaptability. We press on.
This is not metaphor. Prospect theory tells us people think in relative terms, not absolute ones. Winter and Parker (2007) showed that patients currently experiencing illness are significantly more likely than healthy patients to prefer aggressive life-sustaining interventions—not because they're irrational or poorly informed, but because their reference point has shifted. The distance between disability and death looks different when you're already living with disability. Healthy people consistently underestimate the value they would place on life in diminished states of health. The Sudore and Fried (2010) paper in the Annals of Internal Medicine made this the centerpiece of their argument for redefining ACP: the objective should be preparing patients and surrogates for in-the-moment decision-making, not pre-specifying treatment preferences that will be applied to a version of the patient who no longer exists.
Preference instability isn't a bug in ACP. It's a feature of being human. And it's exactly what a checkbox cannot capture.
It also calls into serious question the "DNR" that you joke about (I hope...) tattooing on your chest.
What ACP Should Actually Do
If the checkbox is broken, what works?
Two things have durable value in ACP. The first is identifying who the surrogate decision-maker is—and not just naming them, but preparing them. The second is understanding how the patient thinks about health and makes medical decisions. Not what they would choose in hypothetical scenario X or Y. How they think. What they value. What trade-offs they can and cannot tolerate. How they've made difficult decisions in the past. Whether they want to be shielded from hard truths or told everything, even when it's grim.
Rebecca Sudore's PREPARE for Your Care program is the closest thing we have to an evidence-based model that gets this right. In randomized trials with over 1,400 English- and Spanish-speaking older adults, 98% of participants engaged in some form of advance care planning. The PREPARE website plus an easy-to-read advance directive increased self-reported goal-concordant care from 33% to 59% and reduced disparities among patients with limited health literacy and Spanish-speaking populations. Crucially, PREPARE doesn't ask patients to predict future treatment preferences. It prepares them to communicate values and needs when a decision must actually be made. It also increased patient empowerment by 41% and clinician responsiveness by 51% in audio-recorded primary care visits.
The "starting point" argument matters here. The best ACP gives a specialist palliative care team somewhere to begin a conversation, not a destination to enforce. "When you talked to your PCP, you told her that being at home mattered more to you than length of life. How are you thinking about that now?" That question—how are you thinking about that now—is doing the work. It acknowledges that the plank may have been replaced. It invites the patient to tell you whether the ship is still the same.
Behavioral economics, applied constructively rather than as a critique, points toward designing ACP systems that work with human decision-making rather than against it. A 2020 paper in the Journal of Palliative Medicine outlined how defaults, social norms, and nudges could enhance ACP interventions. But there's a critical distinction between a nudge that gets someone to fill out a form and a nudge that gets someone to sit down with their daughter and say, "If I can't speak for myself, here's how I think about these things, and here's the room I want you to have to make a judgment call I can't predict." One produces documentation. The other produces preparation. CMS is proposing to measure the first.
(For what it's worth: my own advance directive doesn't say a word about CPR or intubation. It has a values addendum that says what quality of life means to me, who I trust to interpret that in-the-moment, and—just like my mama says—that I will haunt anyone who willfully disregards my wishes.)
Where I Might Be Wrong
The CMS measure hasn't been finalized. I hope that the documentation requirements could turn out to be more substantive than checkbox. If CMS defines "high-quality ACP" in a way that requires values elicitation, surrogate identification, iterative conversation, and evidence of preparation rather than a one-time documentation event, the measure could be a net positive. The final rule matters more than the proposal.
The preference stability literature is more nuanced than the argument above implies. Skolarus and colleagues, using NHATS data, found that national end-of-life treatment preferences were relatively stable from 2012 to 2018. I think that the instability I'm describing is more about individual patients navigating actual illness trajectories rather than population-level trends. Both things can be true.
My comfort with iterative, in-the-moment decision-making is shaped by my training and access to specialist palliative care. Patients who don't have access to a palliative care team—which is most patients with serious illness in America—may benefit from having something documented, even if it's imperfect. A flawed advance directive that gets a surrogate into the room is still better than nothing at all. I don't want the perfect to be the enemy of the functional.
And Morrison may be right that at some point, the field's continued investment in ACP represents an opportunity cost: resources that could go to building better care delivery models, addressing disparities in access, and training more clinicians in serious illness communication. I don't think the answer is to stop doing ACP. I think the answer is to stop measuring the wrong version of it and start building systems around the version that works.
The Ship That Keeps Sailing
The question isn't whether to do advance care planning. The question is whether we're willing to do it in a way that honors how human beings actually make decisions: under uncertainty, with shifting reference points, with selves that change as illness changes them.
A quality measure that counts whether a conversation was documented is measuring the shadow, not the substance. What we need—what patients and surrogates and clinicians actually need—is a system that prepares people to navigate decisions they can't yet imagine, with the humility to acknowledge that the person making the decision may not be the person who made the plan.
Sudore and Fried got this right fifteen years ago: the objective of advance care planning should be preparation for in-the-moment decision-making, not the pre-specification of treatment preferences based on hypothetical information. PREPARE works because it takes this seriously. The CMS measure, as currently proposed, does not.
We can do better than a checkbox. We can build systems that ask the right questions: Who do you trust to speak for you? How do you think about trade-offs? What does a life worth living look like to you right now—and how might that change? What room do you want your surrogate to have when you can't weigh in yourself?
These are harder to measure than whether a form exists in an EHR. They're also the only questions that matter when the ship has been rebuilt and someone has to decide where it sails next.
I am a palliative care physician, educator, and professional strategery expert. Known for turning rounds into rants and rants into teaching points. Rounds & Rants represents my views — not those of any institution or professional membership organization where I hold a role. I don't write on their behalf and they don't vet what I publish.



